

Recently I was on a panel discussion on neuroscience datasets at a premier engineering institute. The discussion was part of a symposium on Data-driven innovations. As the meeting was held when semester examinations were going on for the students of the institute, most of the audience were external students from neighboring state-run engineering colleges. My fellow panelists were a neurosurgeon who was into startup ecosystem and a neuro-opthalmologist who was collaborating with the host institute.
As I introduced myself as a neurologist working on stroke and sleep, the panel got a barrage of questions on sleep and dreams, almost disturbing the topic of the discussion. There were questions on why we dream, why certain dreams we can recollect and certain others we cannot, why we have a feeling that some events in dreams have already had happened and so on and so forth. After the meeting there was questions on the sidelines of the meeting whether dreams (during sleep) can turn true or that we can predict our future using dreams. A young man asked what is ‘manase’ in his vernacular depiction of the term. He lamented that he asked many people regarding the ‘stuff’ of mind ( and ? its relationship with body), but none seemed to give clear answers. He wanted to know the nature of ‘manase’.
I did not expect that I need to answer such question in a symposium on data science. It was clearly tangential questions that should have been moderated. But what struck me was that these questions are unresolved among students in their early adulthood.
I think the students find it confusing because there are a lot of pseudoscience and mumbo-jumbo in the online space that people are not able to figure out what is correct and evidence-based and what is not. In most of the academic circles these questions are not clearly answered, and most of the students end up consuming culturally conditioned biased materials that are far from the evidence we have in the scientific literature
Given the importance of these phenomena in our daily lives, let me unpack them one by one.
Why do you sleep?
Sleep is considered a ‘homestatic process’. In common language it is a period of maintenance needed for the brain to restore and refresh its activity.Studies have indicated that glymphatics drainage, a system that clears toxic or unwanted cell structures, functions maximum during sleep. There is also augmentation of brain connections during the process know as ‘synaptic strengthening’, an important activity of improving recall of learned activity.
Studies have found that rats that are sleep deprived for 2-3 weeks tend to die. Also rats that are progressively disrupted of sleep have a higher chance of immune dysfunction and dying of infection.
Sleep requirement for different organisms vary. Rats need to sleep only for few minutes. Human needs to sleep for hours together. This is more or less related to the complexity of the brain structure.
Large mammals like a whale with large brain needs to sleep more. Whales tend to sleep with one hemisphere at a time. In other words they shut down one hemisphere at one time, while the other part of the brain is functioning. This is considered an evolutionary adaptation for preventing predatory attacks during period of prolonged sleep.
Humans too have such evolutionary adaptations. Not all human have similar type to propensity to sleep. Some people have a propensity to sleep early in the night (called larks), while other people have a tendency to sleep late in the night (called owls). This is considered to be an evolutionary adaptation to guard the camping site where a group of tribe would be remain awake, while others will be sleeping. This consititional variation in the propensity for sleep is technically called chronotype. Human needs to sleep more as brain is a high functioning organ. While brain constitute only 2% of body weight, it consumes 20% of oxygen used by the body.
What happens during sleep?
During sleep the brain shut down its normal processing of external and internal sensory information. There is evidence that activity of thalamus, the gateway through which our sensations from the peripheral sensory receptors communicates with the major centres of the brain required for ‘perception’ is different during sleep. During sleep thalamus reduces the sensory inputs to the higher centers of the brain. There is a recent study which shows that brain connectivity is reduced during NREM sleep. In the study when a magnetic pulse was given to the brain of human participants who are in deep sleep (NREM sleep), the pulse activated the brain only locally, while the magnetic pulse administered to waking participants spread widely across the brain. It is also shown that brain’s energy consumption reduces during sleep.
Essentially, brain become less connected and less active during significant part of the sleep (i.e. during the NREM sleep which form 75-80% of normal sleep; We will discuss REM and NREM sleep stages later). It reduces intake of information from our sense organs by acting through the sensory gateway, thalamus.
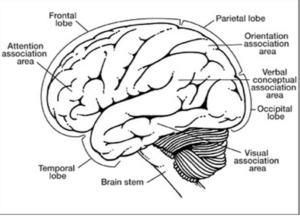
Most of the functions of brain are due to its interconnectivity. Brain can be visualized as a highly interconnected parallel processing computer. Many of our understanding of our world are due to this interconnectability of various regions of brain. For instance, while the sensation of vision is mediated by our occipital cortex in the back side of the brain, our understanding of three dimensional shapes and names of the object in the 3D space is effected by other regions of the brain like visual association area, and areas for colour perception. There is an area in the back side of brain called temporoparetal junction (TPJ) that is important in integrating all the sensory inputs and giving us a sense of ‘self’ and sense of space that is ‘external’ to our self. This ‘sensation’ of self is crucial to the organism to survive.
A brain that is not interconnected, is a brain without any ‘awareness’ of the self and the external world. Sleep is one such situation where our ‘awareness’ become progressively reduced. In this way it is similar to anesthesia given during surgery. But sleep is different from anesthesia in that sleep is an active process automatically put on and off by the body every night and day.
Sleep is effected by two processes. One, an internal clock linked to the day-night rhythm (called circadian clock) and two, by a process called Process S affected by sleep debt or sleep pressure. As you progress through the daytime, brain store of energy gets depleted. As this happens a chemical called adenosine accumulate. Adenosine activates centers connected with sleep to switch on to a ‘sleepiness mode’. Usually this process coincides with the night time of the circadian clock. The circadian clock releases the hormone melatonin when it senses that it is ‘time’ to sleep. While every cell in the body has a clock, an area in the brain called ‘suprachiasmatic nucleus (SCN)’ is a specialised ‘master clock’, that responds to light signal from the eye and mediates the natural process of ‘sleepiness’ linked to the day-night cycle. However, the Process S itself can activate sleep if the sleep pressure is significant enough. Thus, irrespective of the day-night cycle and the influence of the circadian rhythm mediated by SCN, sleep will be induced is Process S is overwhelming.
The Process of Sleep
As the sleep proceeds, the brain waves become progressively slower. In the wake stage when a person closes her eyes, we can record a brain wave known as alpha. This wave has a frequency of 8-13 per second. As sleep progresses the alpha wave become slower and decrease in height (this process is know technically as ‘alpha drop out’). With this person will enter to stage 1 of Non-rapid eye movement sleep (NREM). After few minutes, the person will proceed to the stage 2 where the brain waves become progressively slower. In stage 2, brain waves shows certain wave forms known as ‘sleep spindles’ and ‘K complexes’.
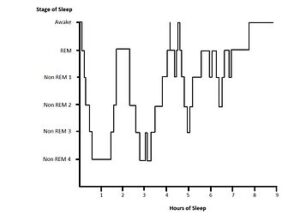
In the next stage the brain waves becomes slower to the range of less than 4 per second. When such slow wave occupies at least 30% of a 30 sec record we call it Stage 3 or N3. This is the deepest phase of sleep. After 90-120 minutes of NREM sleep, the brain waves changes to a state called Rapid Eye Movement (REM) sleep. At this stage, our eyeballs start to move rapidly to and fro, muscles become paralyzed and brain waves show a pattern similar to wake state. This stage is also called as paradoxical sleep. It so called because brain waves appear as if the person is wake. If people are woken up at the REM sleep, they have high probability to recollect dreaming. Studies on REM sleep has shown that this is time in which people dream. Although dreams have been documented during NREM sleep as well, REM sleep is associated with vivid dreaming. Brain connectivity analysis during REM sleep has not been done. But it is expected that during REM sleep there would be increased brain connectivity similar to wake state.

Sleep runs through these 45-60 minute cycles. As sleep progresses the proportion of NREM sleep decreases and REM sleep increases. NREM sleep is considered a maximum quiescent state where the brain tries to recuperate the fatigue causes by the wake hours.
REM stage is considered a state when memory consolidation happens. It is postulated that memory bits are transferred from temporary storage to long term storage during this time.
It is conceivable that when memory bits are transferred it evokes dreams. NREM sleep also generates dreams. But they are not easily recollected. The organised story telling like that happens in vivid dreams is characteristic of REM sleep. It is further conceivable that when the brain is disconnected, ‘story telling like dreams’ are not produced, while during REM state when the brain network reestablish connections spectacular dreams emerges. In fact, if the muscle is not paralyzed like that happens in normal REM state, people will try to enact their dreams – like driving, fighting or whatever they are appearing to do in their dreams. In a brain disorder called REM state behavioral disorder ( RBD) seen in many neurodegenerative conditions like Parkinson’s disease where the normal muscle paralysis of the REM state does not happens , patients tend to enact their dreams often causing self injury or injury to their bed partners.
Dreams
Dreams are the byproduct of cross connection between various brain areas when the memory bits are exchanged. The irrationality of dreams is due to the low functioning state of the time-space-and-reason integrating centres of the brain.
Dreams has a special affinity to weave story around items on which one has special emotional connect. This is because areas of short-term memory storage and areas that control emotions are closely connected. Neuroanatomy refers to this area as the limbic system.
Dream like state can be achieved artificially by manipulating neurotransmitters in the brain. For instance, drugs like 3,4-Methylenedioxymethamphetamine (MDMA) is found to disconnect the brain areas giving us a sense of identity in space. If the brain centre governing our sense of space is disconnected, we feel that we are the whole universe- that there is no difference between self and the external world. Magic mushroom or Psilocybin mushrooms used by indigenous people of Mexico produces such an effect. The space displacing effect of Soma described in Rig Veda is considered to be mushrooms like Amanita muscaria, Psilocybe cubensis, or Claviceps purpurea.

Consciousness, Coma and Sleep
People confuses consciousness as a ‘thing’ that is behind all. Tens and hundreds of texts have been written on the ‘thing’ behind body that oversees body function. However, modern neuroscience does not see a stuff behind brain or body that stays put when the brain or body is not functioning. After an anaesthesia session or a temporary coma like when patients have when there is generalized seizure (generalized seizure occurs when abnormal electrical activity spread across the brain due to various causes, essentially disrupting brain function for a period of time) patient would be unaware of the period of time during which they are in coma. It will be as if a bit of time is erased out of the scheme of ‘consciousness’. In sleep such temporary loss of consciousness happen in a controlled reversible manner. It is purely a network disconnection occurring in a systematic fashion to repair and recuperate brain connections. There is noting mystical in this. In this context, mind is a feeling arising out of network attending to its own senses and surroundings. If the network is abolished, mind will also be abolished.
Philosophers and monks who do not have any understanding of the anatomy or physiology of brain or the pathophysiology of brain dysfunction states, sat in their couch or caves to construct elaborate theories of the mind and body. In that process they had only tool- there own capacity for imagination and theorize on it.
The theory webbed in Mandukya Upanishad is one such mythical misunderstanding. It states that there are 4 states: the wake world, the dream world, the deep sleep state and the fourth one, the turiyam (the 4th). First three states are manifest when the person is awake, dreaming in sleep and in deep state. Mandukya Upanishad states that the fourth one, turiyum underlines all three former states, but cannot be known, heard, felt or inferred. It is the pure consciousness that watches and ‘exists’ through all the former three states. In Y- tube we have a video of a celebrated monk known as Swami Sarvapriyananda articulating such a story to students of IIT- Kanpur. Neither the monk nor his audience seems to know that they are committing a major logical fallacy. The monk says that turiyum is like Higgins Boson particles – you can’t see, hear, learn or infer. But the author of the Upanishad ‘knew’ about it for Sarvapradhanda to interpret it. By the way, he does not qualify whether this Higgins Boson particles is indeed ‘non-inferable’ or ‘non-detectable’ (Without inferring how did they came to know something as existent?) Using false inferences and a series of major logical fallacies, Swami carries his untutored engineering students to eternal confusion.
https://www.youtube.com/watch?v=eGKFTUuJppU&t=1378s
The reason why the validity of the authors of Upanishad is not questioned is because of an axiom delivered to the students of Vedas that the ‘Smritis’ are always true. They are not questionable. Its like Quran or Bible. Descended as ‘words’. (See initial Sukta’s of Brahmasutras) Many of the ancient and medieval so-called argumentative scholars won their debate sessions with the Buddhist monks by invoking this axiom of unquestionability of the Sruthis (the word).
Modern neuroscience, however, does not have any such baggage. Sleep, dreams and feeling of having a ‘mind’ are all the functions of the enormous parallel processing computer of the brain. I think this point of view should be clearly articulated to dispel the confusion created by people who middle in areas of neuroscience based on unverified speculations of philosophical texts. Here, one needs to differentiate what is verified, what is verifiable and what is neither verified nor verifiable.
Modern science and its constructs are either verified or verifiable. Pseudoscience, on the contrary, are neither verified or verifiable. The story of Thuriyam is one such construct. Unless students know of this fundamental differentiation, they get confused in the admixture of science and pseudoscience. The questions that I had to field in the above mentioned symposium is just the tip of the iceberg of an educational system which does not systematically answer questions that trouble everyone as they grow up.
References
1.Newberg A, D’Aquilli Eugene. Why God Won’t Go away: Brain Science and the Biology of Belief. Ballantine Books. New York.
Why does consciousness fade in early sleep?
Ann N Y Acad Sci . 2008;1129:330-4
3. Blanke O and Arzy S. The Out-of-Body Experience: Disturbed Self-Processing at the Temporo-Parietal Junction. Neuroscientist 2005 11: 16
4. Blanke O, Mohr C, Michel CM, Pascual-Leone S, et al. Linking Out-of-Body Experience and Self Processing to Mental Own-Body Imagery at the Temporoparietal Junction. The Journal of Neuroscience, January 19, 2005 • 25(3):550 –557
Hits: 828